Hyponatremia vs Hypernatremia NCLEX Review & Practice Questions
Hyponatremia vs hypernatremia NCLEX topics are among the most tested electrolyte concepts in nursing school and on the NCLEX exam. Understanding sodium disorders is essential because sodium plays a major role in nerve conduction, muscle contraction, and fluid balance throughout the body. This sodium imbalances NCLEX review will help nursing students recognize symptoms, interpret laboratory findings, and prioritize nursing interventions for both conditions.
According to the National Center for Biotechnology Information (NCBI), hyponatremia is the most common electrolyte disorder, affecting approximately 20% to 35% of hospitalized patients. Severe sodium disturbances may lead to seizures, coma, and life-threatening neurological complications. This is why hyponatremia nursing review, hypernatremia NCLEX questions, electrolyte imbalance study guide, and sodium disorders nursing care remain highly important topics for NCLEX preparation.
Introduction to Sodium Imbalances
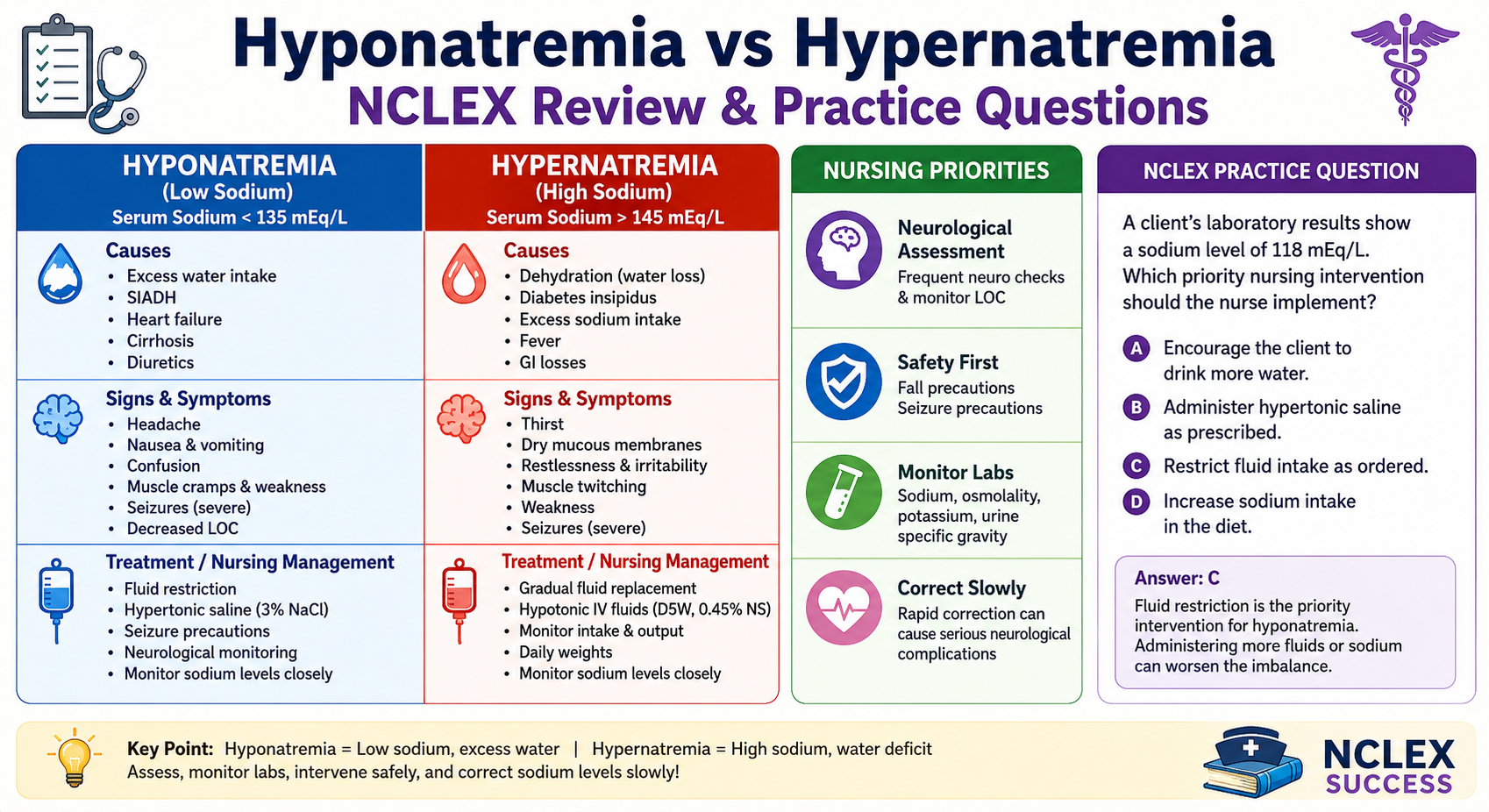
Sodium is the primary extracellular electrolyte responsible for regulating fluid balance, blood pressure, and neuromuscular activity. The normal serum sodium range is 135–145 mEq/L.
- Hyponatremia: Sodium below 135 mEq/L
- Hypernatremia: Sodium above 145 mEq/L
In every hyponatremia vs hypernatremia NCLEX question, students must evaluate how sodium imbalance affects brain function. Because sodium influences water movement between cells, abnormal sodium levels can cause brain swelling or brain shrinkage.
This sodium imbalances NCLEX review emphasizes that low sodium causes cells to swell, while high sodium causes cells to shrink. These changes explain the neurological symptoms seen in sodium disorders.
Severe sodium abnormalities may trigger seizures. Research published in the National Library of Medicine states that seizures are frequently associated with sodium disturbances, especially hyponatremia.
For NCLEX success, students should repeatedly practice hyponatremia nursing review concepts and hypernatremia NCLEX questions because electrolyte disorders often appear in prioritization and emergency scenarios.

Understanding Hyponatremia
Hyponatremia occurs when serum sodium falls below 135 mEq/L. In many hyponatremia vs hypernatremia NCLEX scenarios, low sodium is linked to excess water retention.
Common causes include:
- SIADH
- Heart failure
- Kidney disease
- Excessive water intake
- Diuretic therapy
- Vomiting and diarrhea
This sodium imbalances NCLEX review stresses that elderly patients and hospitalized patients are at high risk for hyponatremia.
Signs and symptoms include:
- Headache
- Confusion
- Lethargy
- Muscle cramps
- Nausea
- Seizures
Severe hyponatremia may result in cerebral edema because water shifts into brain cells. Research shows that, neurological symptoms become more severe when sodium levels rapidly drop below 125 mEq/L.
Nursing priorities include:
- Frequent neurological assessments
- Seizure precautions
- Fluid restriction
- Monitoring serum sodium
- Administering hypertonic saline carefully
This section is essential for any hyponatremia nursing review because rapid sodium correction can cause osmotic demyelination syndrome.
A 72-year-old patient with SIADH becomes confused and develops muscle twitching. Laboratory results show a sodium level of 118 mEq/L. The nurse notes worsening lethargy and nausea. Which nursing action is the priority?
Understanding Hypernatremia
Hypernatremia occurs when serum sodium exceeds 145 mEq/L. In most hyponatremia vs hypernatremia NCLEX situations, hypernatremia results from water loss rather than excess sodium intake.
Common causes include:
- Dehydration
- Diabetes insipidus
- Fever
- Excessive sweating
- Burns
- Inadequate water intake
This sodium imbalances NCLEX review highlights that hypernatremia causes water to move out of cells, leading to cellular dehydration.
Signs and symptoms include:
- Intense thirst
- Dry mucous membranes
- Irritability
- Restlessness
- Muscle twitching
- Seizures
- Coma
Severe hypernatremia may cause brain cell shrinkage and intracranial bleeding. These complications are heavily emphasized in sodium disorders nursing care education.
Nursing interventions include:
- Gradual fluid replacement
- Monitoring neurological status
- Daily weights
- Strict intake and output monitoring
- Administering hypotonic IV fluids carefully
This electrolyte imbalance study guide reminds students that sodium should never be corrected too rapidly because sudden fluid shifts can worsen brain injury
A patient admitted with dehydration has a sodium level of 158 mEq/L. The patient becomes increasingly restless and reports intense thirst. Which intervention should the nurse anticipate?
Key Differences Between Hyponatremia and Hypernatremia
Understanding the key differences between hyponatremia and hypernatremia is essential for answering hyponatremia vs hypernatremia NCLEX questions correctly. Hyponatremia occurs when the serum sodium level falls below 135 mEq/L, while hypernatremia occurs when the sodium level rises above 145 mEq/L.
In hyponatremia, excess water moves into the cells, causing cellular swelling and cerebral edema. This often leads to symptoms such as confusion, headache, lethargy, and seizures. In contrast, hypernatremia causes water to move out of the cells, leading to cellular dehydration and brain cell shrinkage. Patients with hypernatremia commonly experience intense thirst, irritability, restlessness, and dry mucous membranes.
A common mnemonic used in many sodium imbalances NCLEX review resources is “low and slow” for hyponatremia and “high and dry” for hypernatremia. These phrases are frequently included in electrolyte imbalance study guide materials because they help nursing students quickly remember fluid balance changes.
Both conditions can produce severe neurological symptoms because sodium directly affects brain function and nerve conduction. During exams, hypernatremia NCLEX questions and hyponatremia nursing review scenarios often test the nurse’s ability to identify worsening neurological status and prioritize patient safety interventions.
Causes and Risk Factors of Sodium Imbalances
Many hyponatremia vs hypernatremia NCLEX questions focus on identifying risk factors.
Major causes include:
- Diuretics
- Excessive sweating
- Burns
- Vomiting
- Diarrhea
- Kidney disease
- Heart failure
SIADH commonly causes hyponatremia because excessive ADH leads to water retention. Diabetes insipidus commonly causes hypernatremia because inadequate ADH causes water loss.
This sodium disorders nursing care section is important because nurses must recognize underlying causes before implementing interventions. NCLEX exams frequently test elderly patients because aging increases dehydration risk. Older adults often have impaired thirst mechanisms and reduced kidney function. Studies indicate that approximately 5% of the community population experiences hyponatremia, while hospitalized patients have even higher rates.
A patient taking loop diuretics develops confusion and muscle weakness. The sodium level is 128 mEq/L. Which factor most likely contributed to this electrolyte imbalance?
Signs and Symptoms Nurses Must Recognize
Recognizing symptoms early is essential in every hyponatremia vs hypernatremia NCLEX scenario because sodium imbalances can quickly become life-threatening. Early manifestations often include fatigue, weakness, headache, nausea, and mild confusion. As sodium levels worsen, patients may develop severe neurological symptoms such as seizures, decreased level of consciousness, and coma.
This sodium imbalances NCLEX review highlights that neurological complications are the most dangerous because sodium directly affects brain cells and nerve conduction. In hyponatremia, swelling of brain cells can cause cerebral edema, while hypernatremia causes brain cell dehydration and shrinkage.
Muscle-related symptoms frequently include muscle cramps, twitching, and generalized weakness, all of which are commonly tested in hypernatremia NCLEX questions and hyponatremia nursing review materials.
Gastrointestinal symptoms may also appear, including vomiting, abdominal cramping, nausea, and loss of appetite. According to the CDC, approximately 2.9 million adults in the United States live with active epilepsy, emphasizing the importance of seizure prevention in electrolyte disorders. Every electrolyte imbalance study guide stresses that nurses must initiate seizure precautions and closely monitor neurological status in patients with severe sodium abnormalities as part of effective sodium disorders nursing care.
A patient with severe hypernatremia suddenly becomes confused and develops muscle twitching. Which complication should the nurse suspect first?
Diagnostic Tests and Laboratory Findings
Diagnostic testing and laboratory interpretation are heavily emphasized in hyponatremia vs hypernatremia NCLEX questions because nurses must recognize abnormal sodium levels quickly. Important laboratory values include serum sodium, serum osmolality, urine specific gravity, and potassium levels. In most cases, hyponatremia is associated with low serum osmolality, while hypernatremia commonly presents with elevated serum osmolality due to dehydration and water loss.
This sodium imbalances NCLEX review reminds students that laboratory trends are often more important than a single abnormal value. Urine specific gravity is especially useful when evaluating hydration status. High urine specific gravity usually indicates concentrated urine and dehydration, while low specific gravity may suggest fluid overload or excessive water retention.
Many hypernatremia NCLEX questions and hyponatremia nursing review scenarios include multiple electrolyte abnormalities. Nurses should monitor potassium, calcium, and magnesium levels alongside sodium. Every electrolyte imbalance study guide also emphasizes that correcting sodium levels too rapidly can lead to severe neurological complications, making careful monitoring an important part of sodium disorders nursing care.
Nursing Management and Treatment
Nursing management is a major focus in hyponatremia vs hypernatremia NCLEX questions because sodium imbalances can quickly become life-threatening. Treatment for hyponatremia commonly includes fluid restriction, careful administration of hypertonic saline, seizure precautions, and frequent neurological monitoring. In contrast, hypernatremia treatment usually involves gradual fluid replacement, hypotonic IV fluids, daily weights, and strict intake and output monitoring to correct dehydration safely.
This sodium imbalances NCLEX review emphasizes that sodium levels must be corrected slowly because rapid correction can cause severe neurological injury. Safety interventions are also essential and include fall precautions, mental status assessments, seizure precautions, and frequent neurological checks. Research shows that untreated sodium disturbances may rapidly progress to seizures, coma, or permanent brain injury. Because of these risks, hyponatremia nursing review materials and hypernatremia NCLEX questions strongly focus on patient safety and careful monitoring.

A nurse is caring for a patient with chronic hyponatremia. The healthcare provider prescribes rapid sodium correction. Which concern should the nurse report immediately?
NCLEX Tips and Memory Tricks for Sodium Disorders
Every hyponatremia vs hypernatremia NCLEX review should include memory tricks.
Key Mnemonics
- “Low and slow” = hyponatremia
- “High and dry” = hypernatremia
- Neurological status
- Seizure prevention
- Fluid balance
- Laboratory monitoring
This sodium imbalances NCLEX review teaches students to identify life-threatening symptoms first.
Common NCLEX traps include:
- Correcting sodium too quickly
- Ignoring neurological changes
- Confusing dehydration with fluid overload
A strong hyponatremia nursing review should always focus on brain swelling, while hypernatremia NCLEX questions often emphasize dehydration and thirst. Quick comparison reviews are common in every electrolyte imbalance study guide because sodium disorders are easy to confuse under exam pressure.

This hyponatremia vs hypernatremia NCLEX review covered the major differences between low and high sodium disorders, including causes, symptoms, laboratory findings, and nursing management. Both conditions can lead to severe neurological complications if not recognized early. This comprehensive sodium imbalances NCLEX review demonstrated that hyponatremia typically causes cerebral edema and fluid overload symptoms, while hypernatremia commonly causes dehydration and cellular shrinkage.
For NCLEX success, students should repeatedly practice hypernatremia NCLEX questions, focus on hyponatremia nursing review concepts, and master prioritization strategies from every electrolyte imbalance study guide. Understanding sodium disorders nursing care can help nurses identify emergencies quickly and provide safe, effective interventions. Early recognition, accurate laboratory interpretation, and prompt nursing intervention are essential for preventing complications such as seizures, coma, and permanent neurological injury.

No comments yet. Be the first to comment!